Project Overview
OneUM is OncoHealth’s utilization management platform for oncology, designed to review patient treatment regimens and determine their appropriateness. While the platform had grown in scale and complexity, the teams supporting it were struggling with alignment. Documentation was scattered, overly complex, and often misunderstood. Different departments—clinical, product, and engineering—had their own mental models of the service, leading to conflicting priorities, duplicated work, and missed opportunities.
This case study focuses on my work to bring clarity and alignment to OneUM. My role combined research, strategy, and service design: conducting stakeholder interviews, mapping workflows, and creating tools like personas and service blueprints that translated complexity into shared understanding. These artifacts weren’t just documentation—they became living tools that anchored decision-making, improved prioritization, and gave leadership a clear picture of what the service actually delivered.
Through this effort, design became the bridge between siloed teams, helping turn a fragmented process into a cohesive service experience that supported both internal teams and, ultimately, better care for patients.
The Problem

Behind OneUM’s powerful platform was a web of complexity that made alignment difficult. While the system was technically functional, teams struggled with shared understanding and clarity.
Symptoms we uncovered
Documentation confused more than it clarified. It was overwhelming, inconsistent, and rarely used as a source of truth.
Each team had its own version of the service. Clinical, product, and engineering groups all described OneUM differently, which made decisions siloed and conflicting.
New colleagues struggled to onboard. Without a clear explanation of what OneUM offered or how it worked, it was difficult to ramp up quickly.
Duplicated efforts and wasted time. Misaligned projects and duplicated work became common because priorities weren’t connected across teams.
The Impact
Instead of accelerating decision-making, OneUM’s complexity slowed it down. Teams couldn’t confidently prioritize improvements, and the lack of a unified picture meant even leadership struggled to see what the service truly delivered.
Research & Discovery
To move beyond assumptions and surface the root of the misalignment, I started by talking directly with the people most involved in OneUM’s day-to-day. Through stakeholder interviews across clinical, product, engineering, and operations, I uncovered how each group described the service differently—and how those differences created friction. For some, OneUM was a set of clinical workflows; for others, it was a product roadmap or a collection of back-end processes. These fragmented perspectives revealed why alignment had been so elusive.
I supplemented these interviews with surveys to capture broader input, focusing on pain points, bottlenecks, and perceptions of where the service broke down. This helped quantify patterns that individual conversations had surfaced.
Click each persona to view detailed personas.
Click each persona to view detailed personas.






Aligning on Roles
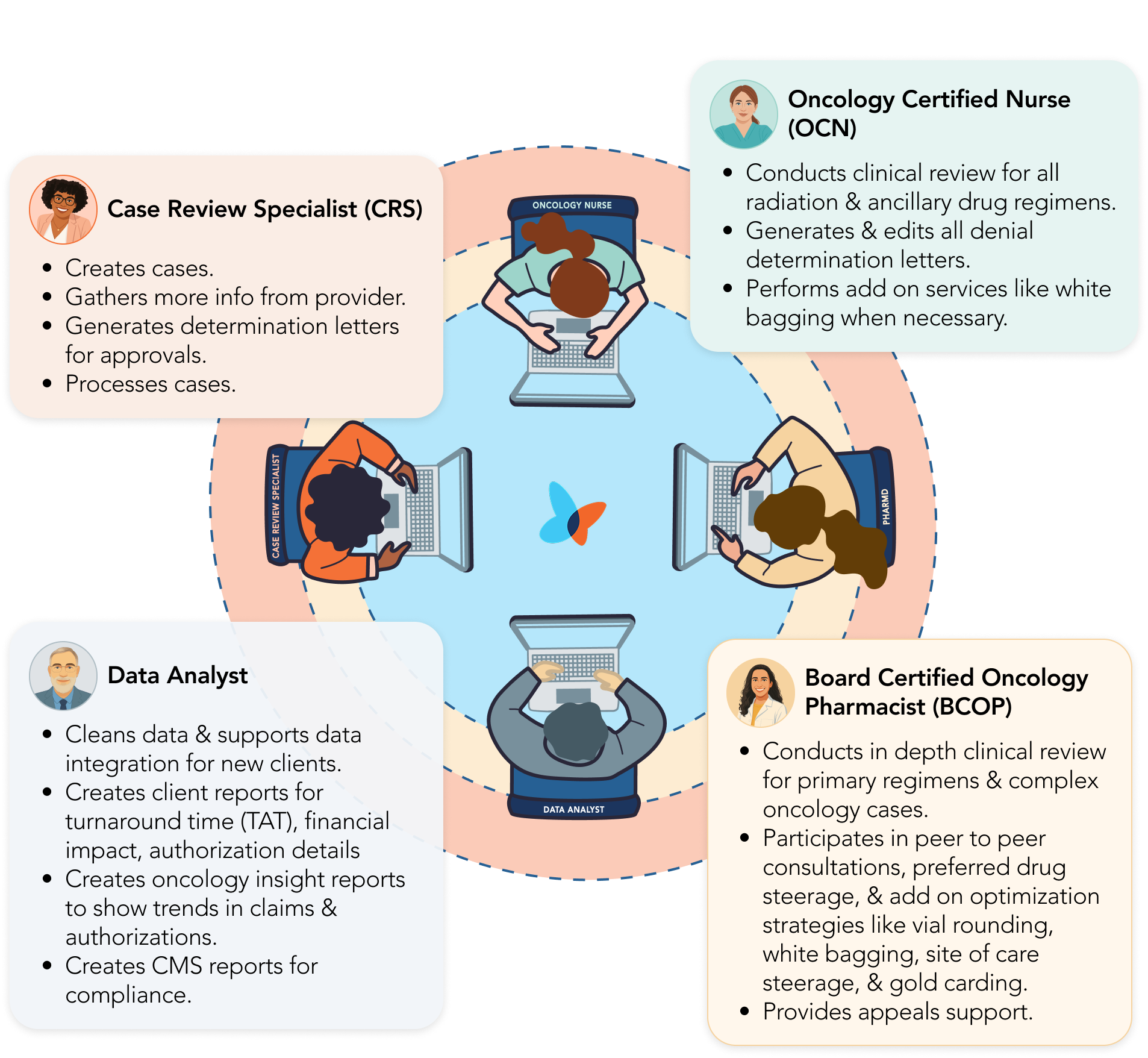
To connect personas to the broader service blueprint, I created a role alignment map. This artifact distilled responsibilities for each key stakeholder in the prior authorization process—case review specialists, oncology nurses, pharmacists, and data analysts—and positioned them in relation to each other.
Unlike the in-depth personas, which captured motivations and pain points, this map zoomed out to highlight roles and responsibilities at a glance. It made it easier for cross-functional teams to see “who does what” and where overlaps or gaps occurred.
Aligning on Definitions
Before I could create the full service blueprint, there was a critical step: aligning on definitions. OneUM was full of specialized terms—PA required, out of scope, NMI, CCF, site of care steerage, vial rounding—that each team used in different ways. What seemed like common language often meant very different things to different groups. Without alignment, even the most carefully designed blueprint risked being misunderstood.
To solve this, I created a visual definitions map that organized these terms within the end-to-end service. Instead of handing out another glossary, I built an artifact that showed where in the process each definition applied and how it connected to downstream steps. This helped teams not only speak the same language, but also see the ripple effects of each decision.

By rooting the conversation in shared definitions, we created clarity before jumping into flows and roles. This artifact became a bridge: it turned abstract terminology into a structured, visual language that everyone could use. With that foundation in place, the service blueprint became far more powerful—because now, every stakeholder was truly looking at the same picture.
From Definitions to a Full Blueprint
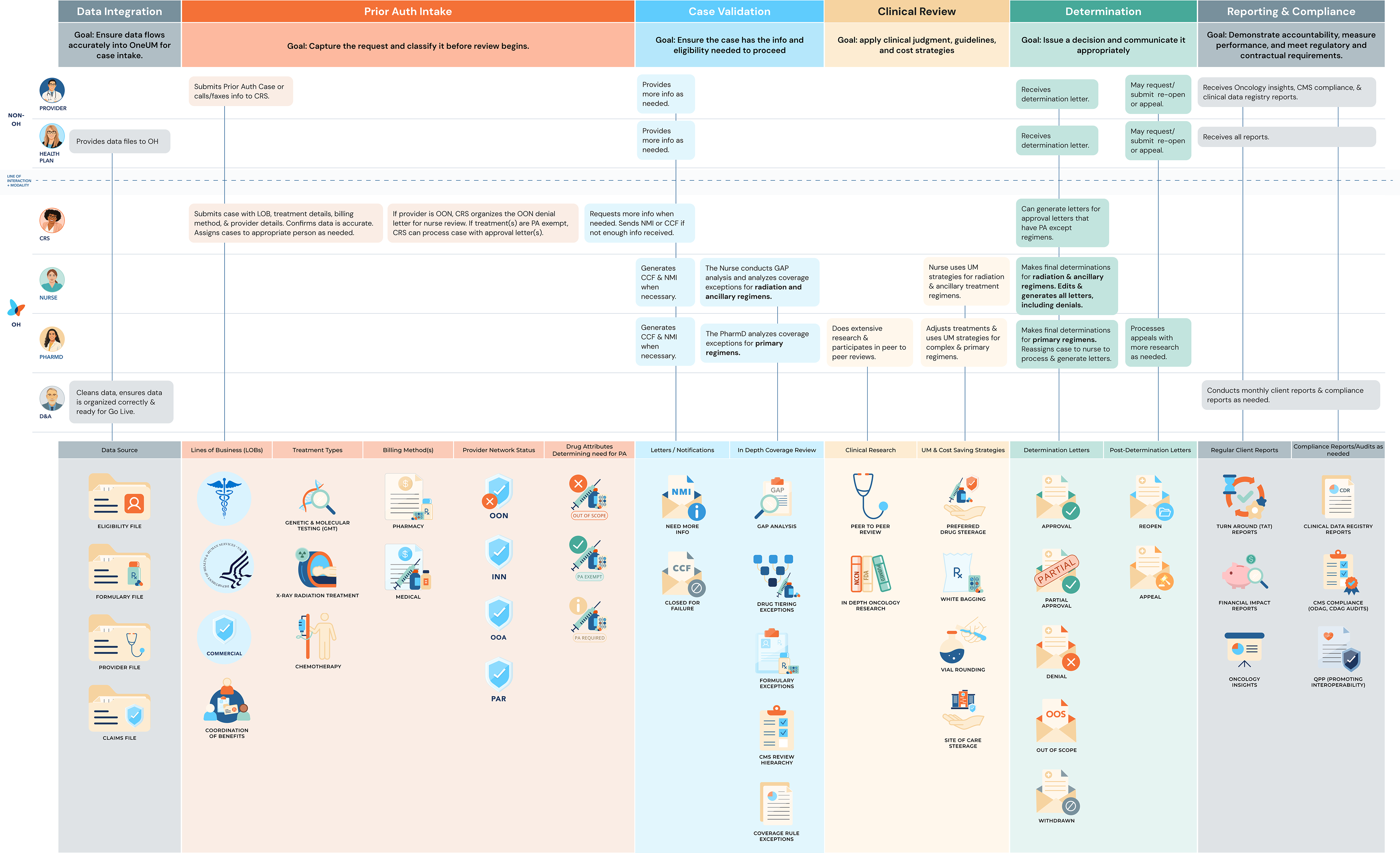
Once roles and definitions were aligned, the final step was to bring everything together in a comprehensive service blueprint. This artifact mapped the entire prior authorization journey—from data integration and intake, through case validation and clinical review, to determinations and reporting.
Unlike the earlier role alignment map (which showed who does what) and the definitions artifact (which clarified what terms mean), the blueprint synthesized it all into a single story. It highlighted when and how roles connected, where definitions applied, and where gaps or redundancies slowed the process.
This blueprint became the backbone for cross-team discussions. By seeing the full journey laid out visually, stakeholders could:
1. Spot inefficiencies and misaligned handoffs.
2. Understand dependencies between clinical, product, and engineering teams.
3. Anchor prioritization discussions in a shared, holistic view of the service.
Together, the personas, definitions, role alignment, and blueprint reframed OneUM from a patchwork of siloed processes into a unified service story.
Impact
While the project was ongoing when I transitioned roles, the artifacts I delivered created immediate value:
Alignment
Teams began referencing personas and the blueprint as common ground in planning sessions.
Clarity
Leadership had a clearer picture of what OneUM actually delivered, making prioritization discussions more focused.
Onboarding
New hires used the blueprint to understand OneUM faster, reducing ramp-up time.
Momentum
By proving the value of service design, I helped shift perceptions of “documentation” from static binders to actionable tools.
“The blueprint finally gave us a way to see the whole process... Seeing gaps and opportunities became significantly easier."
- Director of Pharmacy
Reflection
This project reinforced the power of design as a bridge between siloed teams. I learned how to balance the needs of clinicians, product managers, and engineers by creating artifacts that spoke each group’s language while unifying them around a single narrative.
Most importantly, it showed me that in healthcare—where workflows are complex, regulated, and high-stakes—service design isn’t just about clarity. It’s about building trust, aligning people, and making sure the systems behind the scenes ultimately support better care for patients.